ECR 2017 / C-1945
Fat-containing liver lesions - inside out
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2017
Poster Number:
C-1945
Type:
Educational Exhibit
Keywords:
Abdomen, Liver, Interventional non-vascular, MR, CT, Ultrasound, Biopsy, Neoplasia, Tissue characterisation, Pathology
Authors:
V. Attard1, L. Reichmuth2, J. DeGaetano1, K. Cortis3; 1Msida/MT, 2Tal-Qroqq/MT, 3Zebbug/MT
DOI:
10.1594/ecr2017/C-1945

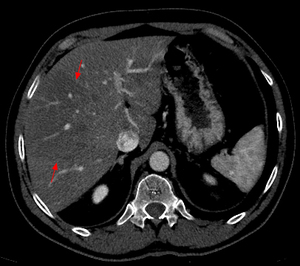
Fig. 1:
Axial computed tomography image shows a large area of regional fat infiltration...

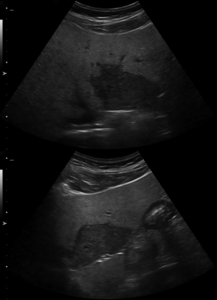
Fig. 2:
Ultrasound images show features of diffuse accumulation of fat in the liver...

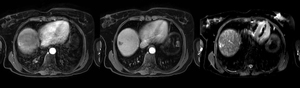
Fig. 3:
Axial T1-weighted opposed-phase image demonstrates diffuse loss of signal with...
 and venous washout (middle image). It is bright on T2-weighted imaging (right image).")
Fig. 4:
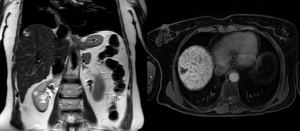
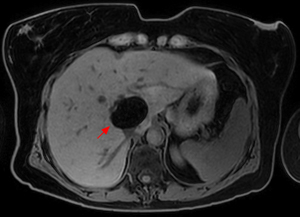
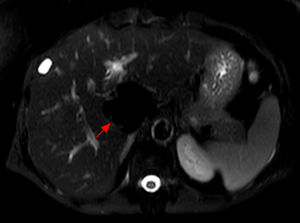
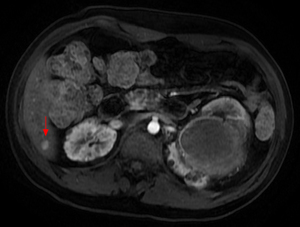
Magnetic resonance images obtained in a 56-year-old lady with primary biliary...
 image demonstrates a high signal intensity lesion in the subcapsular portion of segment VII in a 56-year-old lady with primary biliary cirrhosis.
On delayed-imaging using hepatobiliary contrast agent (right image), a hypointense focal mass is demonstrated in segment VII.")
Fig. 5:
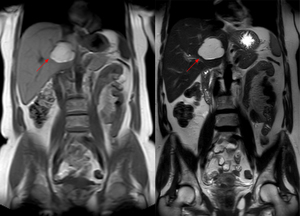
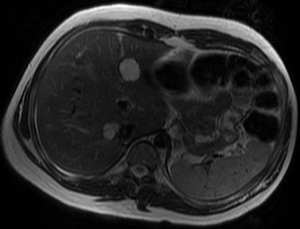
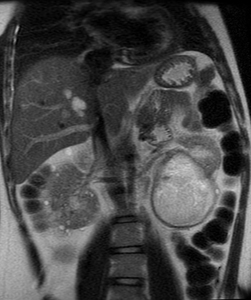
Coronal T2-weighted single-shot fast spin-echo (left) image demonstrates a high...

Fig. 6:
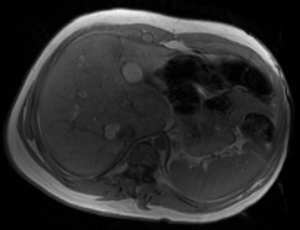
Axial T1-weighted opposed-phase image shows signal intensity loss of the lesion...

Fig. 7:
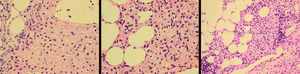
Histological evaluation of the lesion in segment VII shows areas with thick...

Fig. 8:
Routine ultrasonography performed in a 61-year-old lady, shows a well-defined...
 and T2-weighted (right) images there is a hyperintense lesion in segment V of the liver. Findings are in keeping with a hepatic lipoma.")
Fig. 9:
On magnetic resonance, T1 (left) and T2-weighted (right) images there is a...

Fig. 10:
Axial T1-weighted fat-suppressed image demonstrates loss of signal intensity...

Fig. 11:
Axial T2-weighted fat-suppressed image again demonstrates loss of signal within...

Fig. 12:
Axial T1-weighted in- and opposed-phase images demonstrate loss of signal...

Fig. 13:
Axial T1-weighted image demonstrates multiple bilobar well-defined high signal...

Fig. 14:
Axial T2-weighted image demonstrates multiple bilobar high signal intensity...

Fig. 15:
Axial T1-weighted image with contrast demonstrates internal enhancement of one...

Fig. 16:
Coronal T2-weighted single-shot fast spin-echo image demonstrates high signal...

Fig. 19:
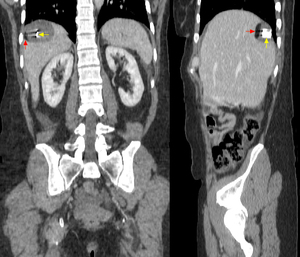
Ultrasonography images obtained in a 42-year-old lady who presented to the...
 and sagittal (right image) reformations demonstrate a well-defined subcapsular rounded lesion in segment VII of the liver. The lesion contains both fat and calcification consistent with a hepatic teratoma.")
Fig. 20:
Coronal (left image) and sagittal (right image) reformations demonstrate a...